
SBI241 Pathophysiology for Healthcare Case Study 2
Case Study
Smith, a 47-year-old male truck driver presents to the emergency department with intractable nausea and vomiting, dyspnoea on exertion, and dizziness. The nausea began about two weeks prior to admission; vomiting has occurred within the last few days. There is no history of medication or toxin exposure. Smith has lost some weight recently and his current body weight is 52 kg. His past medical history is positive for hypertension diagnosed 14 years ago with no follow-up. He has smoked 1 packet per day for 27 years.
On physical examination, his blood pressure is 160/120 mmHg, temperature 36.7°C, pulse 100/min. His skin is pale with numerous areas of bruising and excoriations. Chest x-ray shows moderate cardiomegaly with increased pulmonary vascular markings and hazy obliteration of the lower lung bases. Abdominal ultrasound examination shows a right kidney size of 7 cm and a left kidney size of 6.8 cm (normal kidney size approx. 10 cm).
Please answer the following TWO questions:
la. What is the pathophysiological basis of renal changes in long-standing hypertension?
lb. How has this patient developed hypocalcaemia?
(500 words approx.)
2. Based on the clinical picture and laboratory investigations provided, what stage of chronic kidney disease this patient is in and what will be the main management approach at this stage?
(300 words approx.)
Support your answers with appropriate evidence (references). This assignment tests your ability to search scientific literature and present your answer in a scientific language. DO NOT quote lecture notes or your textbook as reference. CDU library has heaps of resources to support you. Please make full use of these helpful resources:
TIPS ON ACADEMIC/SCIENTIFIC WRITING: nttos://www.cdu.edu.audibrary/lanquaqe-and-learning-support/study-skillsiwriting
AVOIDING PLAGIARISM:
httos://www.cdu.edu.au/librarv/lanquaqe-and-learninq-support/study-skillsiacademic¬y
A clinical case study will be provided to you (related to kidney disease) and a couple of questions will be asked. You will have to do scientific literature search to answer the questions.
Support your answers with appropriate evidence (references). This assignment tests your ability to search scientific literature and present your answer in a scientific language. CDU library has heaps of resources to support you. Please make full use of these helpful resources:
Tips on academic/scientific writing: frittps/www.cdu.edu.auflibrarvilanQuage-and-leaming-support/study-skills/w..___ig Avoiding plagiarism:
https://www.cdu.edu.au/libraryilanquage-and-learning-support/studv-skills/academic-integrity
APA referencing guide attps://libquides.cdu.edu.au/cdureferencineapa
HTN has been underway for a long time and takes sustained damage to the renal vasculature, ultimately causing chronic kidney disease (CKD). Since the sustained elevation in blood pressure is a cause of elevated systemic vascular resistance, it places excessive strain on renal arteries and capillaries. This leads to endothelial dysfunction in time and reduce nitric oxide availability as well as promoting vasoconstriction (Nemtsova et al. 2023). Glomerular hyperfiltration as a consequence of the persistent high pressure leads to capillary wall thickening and podocyte injury. Therefore, glomeruli develop sclerosis leading to impaired function of their filtration.
Renal ischemia also simultaneously triggers inflammation and fibrosis in the tubulointerstitial space and accelerates nephron loss. The RAAS is activated; this damage is compounded by the perpetuation of sodium retention and hypertension accelerating kidney dysfunction to CKD progression (Berede et al. 2022). Sustained high blood pressure induces glomerular hyperfiltration and endothelial damage which is a key feature of hypertensive kidney disease through primary mechanism.
● Hypertensive Nephrosclerosis: Arteriosclerosis of renal arteries also results from chronic HTN because of thickening and narrowing of the afferent arterioles. This decreases renal perfusion which leads to ischemic nephron injury.
● Glomerular Hypertension & Hyperfiltration: Hyperfiltration and podocyte injury secondary to increased systemic pressure elevating glomerular capillary pressure to cause glomerulus’s.
● Tubulointerstitial Fibrosis: Inflammatory cytokines release from ischemic glomeruli contribute to fibrosis of the tubulointerstitial space and progressively impair renal function.
Decline in Renal Function:
• The result is glomerular atrophy along with the loss of nephrons,for MBA assignment expert among other reasons, lowering GFR.
• Additionally, further perpetuates HTN by causing impaired sodium handling and activation of the renin-angiotensin-aldosterone system (RAAS).
These changes progress such that over time proteinuria, hematuria, and relentlessness loss of kidney function occur, which can end up in CKD.
1b. Development of Hypocalcemia in This Patient
Hypocalcemia in CKD patients, such as this case, arises due to multiple factors:
Impaired Vitamin D Activation:
The kidneys convert 25-hydroxyvitamin D into its active form, calcitriol (1,25-dihydroxyvitamin D). In CKD, this process is impaired, leading to reduced intestinal calcium absorption.
Hyperphosphatemia:
CKD results in reduced phosphate excretion, causing hyperphosphatemia. Excess phosphate binds to calcium in circulation, decreasing serum calcium levels (Sharifi et al. 2023).
Secondary Hyperparathyroidism (SHPT):
Low calcium and high phosphate levels stimulate parathyroid hormone (PTH) secretion. Chronic PTH elevation leads to bone resorption but does not fully correct hypocalcemia due to resistance to PTH in CKD.
Skeletal Resistance to PTH:
In advanced CKD, bone tissue becomes resistant to PTH, impairing calcium mobilization and contributing to persistent hypocalcemia.
Metabolic Acidosis:
CKD-associated acidosis changes bone buffering capacity, increasing the loss of calcium and worsening hypocalcemia.
Together these mechanisms contribute to the low serum calcium levels in the patient that may result in neuromuscular symptoms, bone pain and increased fracture risk. As in brain and muscles, calcium deficiency causes the exaggerated excitability of neurons and neuromuscular symptoms including muscle cramps, tetany, and paresthesia (Bounds et al., 2022). Sensitivity to fracture is also increased because osteocalcin and osteoporosis may be associated with chronic hypocalcemia. Furthermore, prolonged SHPT, will result in vascular calcification and cardiovascular complications.
Hypocalcemia needs to be managed with controlling these causes including the supplementation of vitamin D to enhance calcium absorption, phosphate binders to reduce phosphate levels and acidimetric to control PTH secretion and maintain calcium homeostasis and to prevent complications that could include neuro muscular symptoms, bone pain and increased fracture risk. To manage hypocalcemia, one should treat the underlying causes (vital D supple and SHPT) and control phosphate.
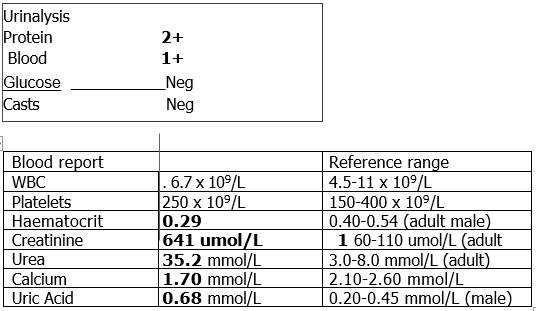
Based on the patient’s clinical presentation and lab values:
● Elevated creatinine (641 µmol/L) and urea (35.2 mmol/L) suggest significantly reduced kidney function.
● Reduced kidney size (<7 cm) indicates chronic structural damage.
● Urinalysis findings (proteinuria, hematuria) and low hematocrit (0.29) support CKD diagnosis.
Using the KDIGO CKD classification:
● GFR Estimation: Although GFR is not explicitly provided, the high creatinine level suggests an eGFR <15 mL/min/1.73m².
● Stage Classification: The patient is likely in Stage 4-5 CKD (severe to end-stage renal disease, ESRD).
Management Strategies:
Blood Pressure Control:
Target BP <130/80 mmHg using ACE inhibitors or ARBs to slow progression.
Electrolyte and Mineral Management:
Phosphate binders to lower serum phosphate levels.
Active vitamin D (calcitriol) to correct hypocalcemia and suppress PTH.
Anemia Management:
Erythropoiesis-stimulating agents (ESAs) and iron supplementation for anemia.
Lifestyle and Dietary Changes:
Protein restriction (0.6-0.8 g/kg/day) to reduce nitrogenous waste.
Low-sodium, low-potassium, and phosphate-restricted diet.
Dialysis or Kidney Transplant Consideration:
If GFR falls below 15 mL/min, dialysis (hemodialysis or peritoneal dialysis) or kidney transplantation should be discussed.
This patient presents with hypertensive nephrosclerosis leading to CKD stage 4-5, with secondary complications like hypocalcemia and anemia. Chronic hypertension has caused significant renal damage, resulting in reduced kidney function, proteinuria, and electrolyte imbalances. The patient’s condition requires a multidisciplinary approach to prevent further decline and manage complications effectively. Blood pressure control with ACE inhibitors or ARBs is essential to slow disease progression (Alcocer et al. 2023). Electrolyte balance must be maintained through phosphate binders and vitamin D supplements to correct hypocalcemia. Anemia management includes erythropoiesis-stimulating agents and iron therapy. Given the severity of CKD, renal replacement therapy options such as dialysis or kidney transplantation should be considered to sustain life and improve quality of life.
Alcocer, L. A., Bryce, A., De Padua Brasil, D., Lara, J., Cortes, J. M., Quesada, D., & Rodriguez, P. (2023). The pivotal role of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers in hypertension management and cardiovascular and renal protection: a critical appraisal and comparison of international guidelines. American Journal of Cardiovascular Drugs, 23(6), 663-682. https://link.springer.com/content/pdf/10.1007/s40256-023-00605-5.pdf
Berede, G. (2022). Pathophysiology, Diagnosis and Management of Chronic Kidney Disease. Journal of Diabetic Nephropathy and Diabetes Management, 1(1), 1-12. https://lsmu.lt/cris/bitstreams/f4fda96c-3ea3-4394-95a6-dc50d70eba94/download
Bounds, L., McGrath, F. and Taubert, M., (2022). Hypercalcaemia to hypocalcaemia: tetany as a side effect of intravenous bisphosphonate treatment. BMJ Case Reports CP, 15(4), p.e249141. https://pmc.ncbi.nlm.nih.gov/articles/PMC9058685/pdf/bcr-2022-249141.pdf
Nemtsova, V., Vischer, A. S., & Burkard, T. (2023). Hypertensive heart disease: A narrative review series—Part 1: Pathophysiology and microstructural changes. Journal of clinical medicine, 12(7), 2606. https://www.mdpi.com/2077-0383/12/7/2606/pdf
Sharifi, A., & Rousta, F. (2023). Hypocalcemia: Why does this happen after thyroidectomy?. Eurasian Journal of Chemical, Medicinal and Petroleum Research, 2(4), 329-339. https://www.ejcmpr.com/article_183266_852357dacf05227a5d7ed28e349d7378.pdf



Essay: 10 Pages, Deadline: 2 days
They delivered my assignment early. They also respond promptly. This is excellent. Tutors answer my questions professionally and courteously. Good job. Thanks!
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
Report: 10 Pages, Deadline: 4 days
After sleeping for only a few hours a day for the entire week, I was very weary and lacked the motivation to write anything or think about any suggestions for the writer to include in the paper. I am glad I chose your service and was pleasantly pleased by the quality. The paper is complete and ready for submission to the professor. Thanks!
![]() User ID: 9***85 United
States
User ID: 9***85 United
States
Assignment: 8 Pages, Deadline: 3 days
I resorted to the MBA assignment Expert in the hopes that they would provide different outcomes after receiving unsatisfactory results from other assignment writing organizations, and they genuinely are fantastic! I received exactly what I was looking for from this writing service. I'm grateful.
![]() User ID: 9***55
User ID: 9***55
Assignment: 13 Pages, Deadline: 3 days
Incredible response! I could not believe I had received the completed assignment so far ahead of the deadline. Their expert team of writers effortlessly provided me with high-quality content. I only received an A because of their assistance. Thank you very much!
![]() User ID: 6***15 United
States
User ID: 6***15 United
States
Essay: 8 Pages, Deadline: 3 days
This expert work was very nice and clean.expert did the included more words which was very kind of them.Thank you for the service.
![]() User
ID: 9***95 United
States
User
ID: 9***95 United
States
Report: 15 Pages, Deadline: 5 days
Cheers on the excellent work, which involved asking questions to clarify anything they were unclear about and ensuring that any necessary adjustments were made promptly.
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
Essay: 9 Pages, Deadline: 5 days
To be really honest, I can't bear writing essays or coursework. I'm fortunate to work with a writer who has always produced flawless work. What a wonderful and accessible service. Satisfied!
![]() User ID: 9***95
User ID: 9***95

Essay: 12 Pages, Deadline: 4 days
My essay submission to the university has never been so simple. As soon as I discovered this assignment helpline, however, everything improved. They offer assistance with all forms of academic assignments. The finest aspect is that there is also an option for escalation. We will get a solution on time.
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
Essay: 15 Pages, Deadline: 3 days
This is my first experience with expert MBA assignment expert. They provide me with excellent service and complete my project within 48 hours before the deadline; I will attempt them again in the future.
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
